- This Discussion Thread has 29 replies, 18 voices, and was last updated 1 month ago by danait.
-
AuthorPosts
-
-
2024-04-12 at 4:23 pm #12379John-paulKeymaster
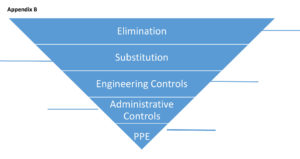
Reflection activity: Thinking of your current or a past workplace provide specific examples of each hierarchy of control – see Appendix B.
-
2026-01-05 at 11:38 am #18119DianeMember
Elimination- commode removed from room that was being shared by 2 clients.
substitution- separate commode per client,
engineered control- each resident with s/s cough cold, c diff isolated or moved to single room.
each room has cart placed outside room with ABHS, Virox towels, PPE supplies, ensure proper signage on entry of room.
administrative control- new policies updated and placed in binders for staff to read. staff huddles used for daily education ensuring all staff every shift is and are aware of new updated IPAC, staff made aware of any new symptoms cough/colds/covid/c-diff /who is on isolation. Staff are also made to self screen before arriving to work, Families emailed and updated if family member is isolated due to symptoms, MD aware of all clients who present with any symptoms.
PPE – Carts placed outside of rooms that are on isolation, reminder to staff at shift report to use proper PPE when entering and exiting rooms, staff are to monitor if bins are low on stock, one staff member who is educated on hand washing, donning and offing of PPE will monitor staff to ensure all steps are performed correctly.-
2026-02-11 at 11:58 am #18499MargaretMember
You provided a very thorough and practical breakdown of the hierarchy of controls in action within your setting. I especially like how you highlighted not only the physical measures like isolation carts and signage, but also the strong administrative strategies such as staff huddles, self-screening, and family communication, which are essential for consistent infection prevention and control.
-
-
2026-01-10 at 8:44 pm #18155Jessica-lynMember
Elimination- Resident with illness being isolated in their rooms. Curtain used to separate rooms with 2 residents. ensuring each resident has their own “bathroom”/Commode.
substitution- separate personal things. Seperate/remove anything that could transport illness.
engineered control- When a resident is sick, they are isolated. If staff is sick they are asked to stay home until they are getting better.
administrative control- Policies are constantly being changed and updated. IPAC education is ongoing and there is always new education being given to the staff. Masks are mandated in the winter months when influenza is higher. Staff also self screen at our home and if sick are asked to stay home.
PPE – PPE is always stocked. When a resident is on isolation, bags and hung from the door that is full of PPE.-
2026-02-06 at 11:03 am #18462SheilaMember
You provided a clear and practical breakdown of the hierarchy of controls. Isolating ill residents and ensuring separate personal items effectively reduces exposure, while engineering controls such as isolation and keeping symptomatic staff home help limit spread. Your administrative controls highlight the importance of ongoing IPAC education, updated policies, seasonal masking, and staff self-screening. Consistent access to well-stocked PPE at isolation rooms further supports safe care and staff compliance.
-
-
2026-01-12 at 10:34 am #18161IbikemiMember
Elimination- Screening visitors and staff for symptoms and not allowing symptomatic individuals to enter the facility. E.g cancelling non-essential in-person meetings or appointments during an outbreak.
Substitution-Using alcohol based hand rubs instead of soap and water when hands are not visibly soiled to reduce contact, and also using safer disinfectants that are effective but less irritating to staff.
Engineering control- By installing physical barriers (plexiglass) at the reception desk. Also, hand-free Sink, soap dispensers, and waste bins.
Administrative control- This can be done by implementing IPAC policies and procedures( hand hygiene, isolation protocols).
Personal Protective Equipment-By wearing gloves, masks, face shields and eye protection when providing resident care.-
2026-01-25 at 10:19 pm #18340RachelMember
Screening staff and visitors with symptoms is the best and most effective way on the hierarchy of control as you are ensuring that anyone who is entering the home has no symptoms, ensuring that the residents and patients are not coming into contact with anyone who is sick and that staff and visitors are not spreading their microbes throughout the home putting staff and residents at risk for illness. By wearing PPE staff are protecting themselves at they are limiting portal of entry with themselves when they are coming into contact with the isolated resident. This helps to stop the spread of infections from resident to staff.
-
-
2026-01-12 at 4:40 pm #18170Rebekah JoyMember
In my workplace as a nurse, I have seen the hierarchy of control used to keep everyone safe.
Elimination: Limiting visitors reduced the risk of infection.
Substitution: Using safety needles instead of regular needles helped prevent injuries.
Engineering Controls: Hand sanitizer stations and isolation rooms helped control infection spread.
Administrative Controls: Policies, training, and infection control guidelines were followed.
PPE: Nurses used gloves, masks, gowns, and face shields when needed.-
2026-02-03 at 10:39 am #18434AlexandraMember
It sounds a lot like the controls in place at my facility as well. I think that things like safety needles are especially helpful for preventing spread of infections even when it someone doesn’t seem sick and you may not be as conscious of potential spread of organisms.
-
2026-02-19 at 5:36 pm #18549AdeyemiMember
Rebekah Joy, I strongly agree with you. In my place of work, during this season, infection outbreaks were limited and brought under control by a high level of compliance with the use of PPE by staff and visitors. Also, by shutting doors of the units under isolation, wandering by residents across units was reduced and the spread of infection curtailed.
-
-
2026-01-12 at 5:48 pm #18173SvetlanaMember
Elimination: Resident with illness being isolated (COVID 19)
Non-essential activity and procedures were cancel.
Substitution: Instead to use nebulizer use metered-dose inhaler.
Engineering Controls: Install hand sanitizer station in the room, soap dispenser and hands-free sinks.
Administrative Controls: Staff education and IPAC training. apply signage on the Resident door with information of airborne contact precautions, limit staff entry.
PPE: Staff to use N 95mask, gowns, gloves and face shields. -
2026-01-15 at 12:14 am #18187danaitMember
Elimination- Clorhexidine wash twice a day to eliminate MRSA
Substitution- Using single use medical equipments
Engineering control- hands-free sinks and ABHRs, contact precaution signage
Administrative control- Screening every patients up on admission to rule out MRSA, hand hygiene audits and training of staff on MRSA transmission
PPE- Gloves and gowns for everyone entering a patient’s room with MRSA, correct use of hand hygiene techniques. -
2026-01-16 at 10:01 am #18196KimberlyMember
Elimination- provided designated vitals machine, bedside commode, and stethoscope to an isolated patient in a ward room instead of sharing the same equipment with a non isolated patient.
Substitution- ensuring isolated patients in ward rooms have designated equipment.
Engineering Controls- Having correct cleaning agents (chlorhexidine, bleach, alcohol) if designated equipment needs to be removed and properly cleaning the equipment.
Administrative Control- providing staff/visitors with IPAC policies and procedures. Ex, providing the education to enhance awareness of infectious diseases, modes of transmission and breaking the chain. Also having the proper signage posted outside room and on curtain.
PPE- Having accessible PPE, ensuring supplies are always stocks with appropriate PPE corresponding to signage. -
2026-01-16 at 3:31 pm #18202AdeyemiMember
In my workplace as a nurse, the following practices are examples of hierachy of controls in the implemented in the workplace:
Elimination: Sterilizing medical equipment with appropriate chemicals after use with a patient
Substitution: Placing sick (persons infected with contagious diseases) in isolation
Engineering controls: Negative pressure rooms to isolate people with diseases like tuberculosis.
Administrative controls: Continuous training for staff on awareness of infectious disease and their prevention, relevant signage in the facility providing reminders on actions to take to prevent spread of infections.
PPE: Carts place in front of doors of rooms of patients in isolation due to infection. Carts are always filled with singe use gowns, surgical face masks and N92, gloves, face shields. These carts are always restocked when supplies are low . -
2026-01-22 at 10:42 am #18303KatrineMember
Examples based on my role as a visiting nurse
Elimination: Physically remove the hazard
– Screening clients by phone before the visit and cancelling or postponing non-urgent visits if the client has symptoms of an infectious illness
– Asking household members with symptoms to leave the room or home during the visit, if possibleSubstitution: Replace the hazard with something safer
– Using needleless IV systems instead of needles to reduce expose to bloodborne pathogens
-Using prefilled medication syringes instead of drawing up medications in the homeEngineering controls: Isolate people from the hazard
-Performing care in a well ventilated area of the home
-Using sharps containers to prevent needle-stick injuriesAdministrative controls: Change the way people work
-Implementing policies and procedures for routine practices and additional precautions
-Training visiting nurses on IPAC protocols, hand hygiene, and donning/doffing PPE
-Scheduling visits to see lower-risk clients first and higher-risk or symptomatic clients lastPersonal protective equipment: Protect the worker with the equipment
-Wearing gloves during wound care, personal care, or contact with body fluids
-Wearing gowns when there is a risk of contact with bodily fluids or contaminated surfaces-
2026-01-25 at 9:02 pm #18338MunazzahMember
Thank you, Katrine. For visiting nurses, the hierarchy of control is essential because of the uncontrolled home environments. Pre-visit screening and postponing non-urgent visits in case of infectious illness eliminates exposure before visit. Substituting needleless systems and prefilled syringes reduces bloodborne pathogen exposure. Engineering controls such as providing care in the well-ventilated area of the home help isolate hazards. Administrative measures support ongoing safe practices and PPE provides a critical final layer of protection to protect both nurse and the client.
-
-
2026-01-24 at 9:25 pm #18331RachelMember
Elimination: When a unit is in out break to prevent the spread of a virus limit any scheduled activities that were planned by Recreation staff, for example every Fridays the home I work at has BINGO sessions with the whole home by cancelling it your preventing the spread of from one unit that might be on outbreak to another that isn’t, as resident from the unit that isn’t on outbreak will not be coming into contact with residents that could be asymptotic from the unit on outbreak.
Substitution: for someone who has a latex allergy, when providing care switch to non latex gloves to prevent an allergic reaction as well as a silicone catheter to prevent allergic reaction.
Engineering controls: opening windows to allow for proper ventilation during outbreaks, ensuring that floors are well stocked with hand sanitizers and ABHS to disinfect objects after use. For example wiping down a sit to stand lift after use from one resident after use and before using it with another.
Administrative controls: completing IPAC audits (hand hygiene, Donning and doffing etc..) to ensure staff are following IPAC polices to prevent the spread, by doing so you can evaluate the areas that need to be worked on and the IPAC manager can hold learning sessions for staff to help educate for the gaps on learning.
PPE: having proper signage along with PPE for isolated residents, this ensures that the proper PPE is being used to limited the spread from resident to staff.-
2026-01-25 at 8:37 pm #18336MunazzahMember
Thank you, Rachel. The hierarchy of control plays an important role in long-term care facilities especially during outbreak when resident who are already immuno-compromised are now at higher risk. Limiting activities by recreational staff is the most effective strategy to prevent or limit transmission during outbreak as there is a less chance of widespread outbreaks. PPE use serves as a last line of defense when other control cannot fully eliminate exposure.
-
2026-02-01 at 5:12 pm #18413AmandaMember
Reducing/eliminating large group activities during an outbreak is essential is stopping the spread of infection. When an outbreak is unit specific where is work, rec staff try to do smaller group activities for those on unaffected units. They continue to provide 1:1 for those who are ill or set up face time visits with their loved ones to reduce feelings of isolation.
-
-
2026-01-25 at 8:17 pm #18335MunazzahMember
Elimination: isolating a resident on contact precautions to physically remove the carrier of hazard.
Substitution: Replacing reusable blood pressure cuffs with disposable to avoid transmission.
Engineering control: Alcohol based hand rubs outside resident’s rooms to isolate people from the hazard.
Administrative control: posting of outbreak signs on doors of all entrances to let staff/visitors know about the outbreak and what infection control precautions to follow.
PPE: using gloves for wound care protects the staff. -
2026-01-25 at 8:54 pm #18337AlexandraMember
Elimination – Ill staff members and visitors do not come into the home.
Substitution – Ill residents are served meals with single use dishes and cutlery that are disposed of in the resident’s room.
Engineering control- the majority of residents are in private rooms that allow for isolation when needed, there are many hand sanitizer stations in each hallway.
Administrative control- Plenty of signage asking visitors to reconsider visits in they have any of the listed symptoms.
PPE- Mandatory masking while in outbreak status-
2026-01-25 at 9:59 pm #18339RachelMember
By using single use dishes and cutlery you are able to limit having more interactions with the infectious objects by keeping them in the same place as where the reservoir resides. when the isolated resident is done eating, their plates and utensils can be disposed of in a separate waste bin in their room that can be labelled “biohazard” so it can be disposed of properly when full. By limiting interactions with the infected objects you are reduces the risk for it to spread.
-
2026-02-21 at 10:24 pm #18559danaitMember
I strongly support these measures, as they show a clear dedication to protecting residents and staff from infection. Implementing multiple levels of control from elimination strategies to PPE creates a well rounded and effective prevention plan. we use the single use plates at the hospital fro isolated patients as well. Altogether, these actions play an essential role in minimizing the spread of illness within the facility.
-
-
2026-01-28 at 1:53 pm #18364IbikemiMember
Hello Rebecca Joy,
I like how you gave examples from practical examples from nursing practice, especially on isolation for elimination and safety needles for substitution. This is a great explanation which shows ways of how different measures work together to reduce infection risks and keep staffs and resident safe. -
2026-02-01 at 4:51 pm #18412AmandaMember
Elimination: Encouraging visitors and staff who are unwell to stay home, providing increased cleaning/sterilization in home areas, especially high contact areas to reduce the spread
Substitution: single use items to be used rather than reusable.
Engineering Control: hand hygiene, ABHS, mandatory masking in resident care areas for staff and visitors, increasing cleaning, isolating those who are ill,
Administrative Control: Management provides proper education and training for staff, provide/update and ensure staff are following safety protocols, ensure staff are provide with proper PPE and PPE is readily available for staff to use when needed, mask fit testing is done for staff, our home notifies families and caregivers of any outbreaks encouraging visitors to stay home, following recommendations from the local health unit
PPE: Staff to wear required PPE based on infectious agent. Signage is posted outside doors to show whether PPE for contact, droplet or airborne. Ensure you have received mask fit testing for proper N95
-
2026-02-02 at 12:28 am #18426TraceyMember
Hello Amanda
In the facility where I work and experience in other facilities I don’t think education or discussion regarding mask fitting is performed as often as it should. Mask fit testing is something “to get through”. It’s physically uncomfortable to do the test and thoughts of prolonging the mask fit exercise can be exhausting. IPAC leads can be essential here. If I were the tester I would make sure I had all the education possible regarding the masks available at the facility and I would educate the staff. Provide a relaxed atmosphere ensuring the staff members comfort. I would let the staff member know I would be performing an audit while they are on the floor working to ensure the mask they require is always available. Ensuring they remember the right mask for them and where it is located.
-
-
2026-02-02 at 12:07 am #18425TraceyMember
Elimination – Restrict resident visitors to essential only when a home is experiencing an outbreak
Substitution – life enrichment staff co-ordinate convenient face time visits for residents and family
Engineering Controls – transportable air exchange units are implemented in or near resident rooms
when essential visits occurAdministrative – At facility door and staff entry areas implement hand hygiene protocols and
implement level 3 grade masks to be worn upon facility entry– Policy and procedure protocols for visitor compliance, education and adherence to
PPE
– Facilitate IPAC lead availability for visitors and staff where education is required
– Perform audits to establish high risk situations
– Ensures reading materials are available and posted for staff and visitors
– Facilitate follow-up with resident and family councils for suggestions and
ImprovementPPE – IPAC lead performs audits that stations are filled with supplies
IPAC lead is visible within the facility providing education when necessary to visitors and staff -
2026-02-06 at 10:54 am #18461SheilaMember
Visiting Nursing
Elimination: Symptomatic clients or family members are screened before visits, and in-person visits are postponed or converted to virtual visits when infection risk is high, eliminating exposure to the hazard.Substitution: In-person follow-up visits are substituted with telephone or video visits for medication reviews or teaching when physical assessment is not required.
Engineering Controls: Use of physical barriers such as maintaining distance during assessments when possible, improving ventilation by opening windows, and using single-use or dedicated equipment to reduce cross-contamination.
Administrative Controls: Agency policies for infection prevention, hand hygiene protocols, visit scheduling to limit exposure, staff education on IPAC practices, screening tools, and clear procedures for cleaning and disinfecting equipment between home visits.
Personal Protective Equipment (PPE): Use of gloves, masks, eye protection, and gowns as required, especially during wound care, respiratory assessments, or when caring for clients with known or suspected infections.
-
2026-02-07 at 7:43 pm #18467MaameMember
1. Elimination: Removing hoppers from units due to risks of cross contamination and growth of bacteria harboring in the sink if not properly disinfected each time when used.
2. Substitution: For end of life residents that take Hydromorphone every 2 hours butterfly needle inserted subcutaneously so resident doesn’t have to be continously poked with a new needle.
3. Engineering controls: During COVID, residents with COVID shared rooms to prevent the spread of the virus.
4. Administrative controls : Management sending staff email reminders about regulary reviewing policies.
5. PPE: Ensuring resident that is on contact precautions for MRSA has the appropriate PPE items readily avaliable in their caddies located at the front of their door.
-
2026-02-11 at 11:56 am #18498MargaretMember
As an RPN working in the community, elimination can include screening clients for infectious symptoms before home visits and rescheduling non-urgent appointments when illness is present. Engineering controls may involve ensuring proper ventilation in the home during visits and using physical barriers like plexiglass in clinic settings. Administrative controls include following agency infection prevention policies, proper scheduling to reduce exposure risk, and ongoing staff education, while PPE involves wearing appropriate masks, gloves, and eye protection based on the level of risk.
-
-
AuthorPosts
- You must be logged in to reply to this Discussion Thread.